Methods
Design
The consolidated criteria for reporting qualitative research (COREQ) was used to guide the reporting of this study (Tong, Sainsbury, & Craig, 2007). A qualitative, exploratory approach reflecting an interpretive framework (Green & Thorogood, 2018) was considered most appropriate for developing an understanding of Peer Supporters’ perceptions of factors of importance related to voluntary work among carers of people with dementia.
Participants
Participants (n = 40) were recruited from the Norwegian Health Association's yearly meeting for the Peer Supporters at a hotel in Norway. The third author was responsible for recruiting the participants and informed them about the purpose of the study, as well as data collection procedures by mail or post in September 2017. All the volunteers at the meeting attended the focus groups. The Norwegian Health association offers training, follow-up and personal mentoring to each Peer Supporter. The Peer Supporters have experience as carer, spouse or children of a person with dementia. All the Peer Supporters have attended a three-day training program consisting of many topics such as understanding the Peer Support role, how their support is a supplement to the formal primary care service, it is voluntary and based on the Peer Supporters own experiences. They learn about empathetic listening and encouragement, possible coping strategies, how to facilitate a conversation, meeting families in crisis and group management in support groups. The Norwegian Health Association Dementia help line counsellors are mentors and supervisors. They are responsible for the recruiting, the training program and the follow-up. The Peer Supporters are all available for telephone calls from other carers. Their contact details are available on the website of the Norwegian Health Association. Once a year all the Peer Supporters meet to share their experiences. Together they reflect on their experiences and learn from each other.
Data collection
Four focus group interviews were conducted in different rooms. Focus groups enable the exploration of a range of opinions and create opportunities for participants to adjust opinions to others’ reflections and statements in the group (Krueger & Case y, 2009). The authors developed a question guide for the focus groups based on literature and experience. One is a nurse with expertise in dementia (author no. 3), an employee of the Norwegian Health Association and also serves as a supervisor for the Peer Supporters. The topic guide was designed to cover key areas with reference to the aims of the study. A copy of the topic guide is included in Appendix 1.
All interviews were voice recorded and transcribed verbatim in Norwegian and carefully translated in English in collaboration with a professional English speaker. The focus interviews took place on the second day at the hotel in November 2017. The participants did not know three of the interviewers but did know the nurse (author no. 3) from the Norwegian Health Association. The groups were assembled by the nurse and mixed according to gender, relationship, new or experienced Peer Supporter.
Ethics
Prior to data collection, approval was obtained from the Norwegian Centre for Research Data (no. 56300). A letter of invitation to participate in the research was sent by the Norwegian Health Association to all the potential Peer Supporters who were going to attend the yearly meeting. In addition, they were also given information at the beginning of the meeting. Anonymity was ensured because no names were used in any part of the data collection. Socio-demographic data were reported carefully because of the very few members of the Peer Supporter Service in the National Health Association. An informed consent form was signed by those willing to participate in the focus groups.
Data analysis
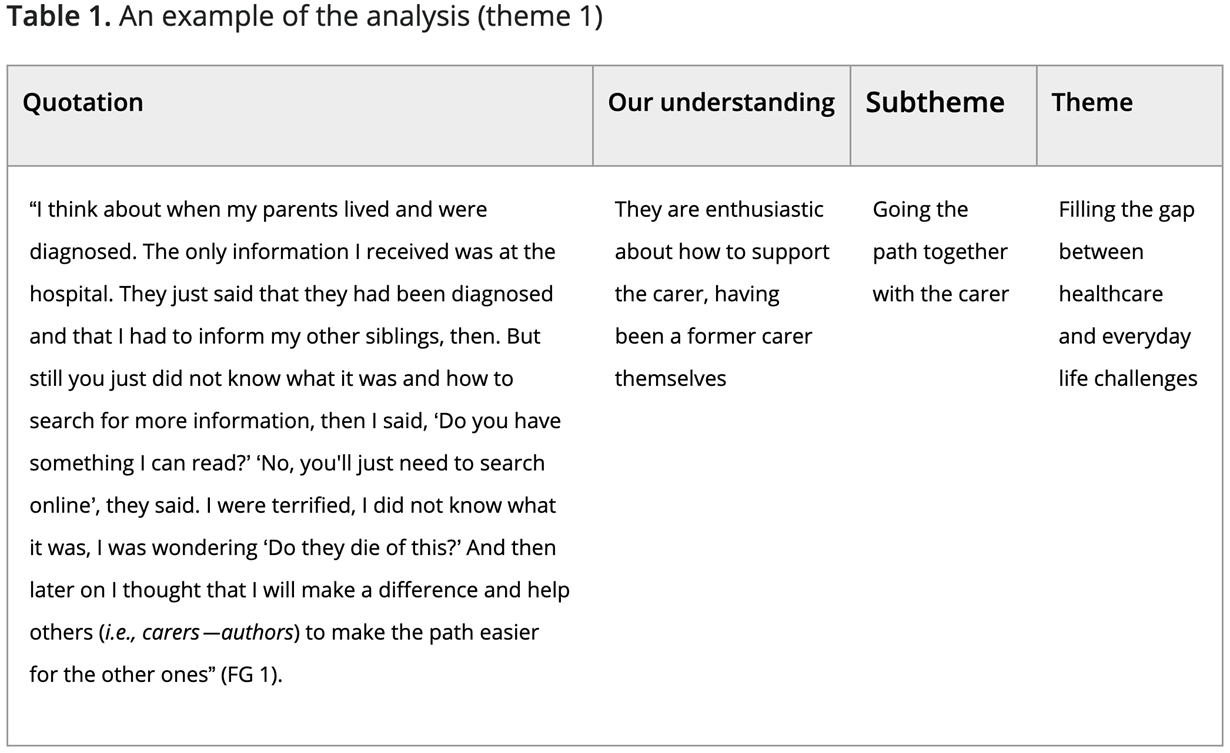
A thematic analysis was undertaken to identify key themes guided by Braun and Clarke’s (2006) phases for analysis. In the first step, the authors read the focus group interviews in an active way, searching for meanings and patterns. The data were then coded and organised into meaningful groups by all authors. The codes were extracted from quotes about Peer Support experiences, and the organised groups were further sorted into sub themes and main themes (Table 1). We can never be entirely free of preconceptions that could influence our interpretation of the data. Therefore, to strengthen the validity, we addressed the criteria of trustworthiness, which include credibility, dependability, confirmability, transferability and authenticity (Guba, 1994). To fulfil this, all the authors made explicit their pre-understanding and existing knowledge about the context and carried out the analysis based on the following six steps of Braun and Clarke (2006).
- Become familiar with the data. All four authors separately read and re-read the transcripts and noted codes. In a face-to-face meeting, all the authors discussed the overall understanding of the data to share understandings and compare them for essential meanings.
- Generate initial codes. All the authors noted initial codes on the transcripts manually and separately. They then met to compare codes and to construct a mutual coding tree.
- Search for themes. We identified central quotations, which we inserted into a common matrix, with these headlines: quote, our understanding, theme and subtheme/candidate theme (Table 1).
- Review themes. The research group met to compare and discuss the themes. We used yellow stickers to highlight themes emerging from each focus group and used a blackboard to summarise the findings. Thereafter, the first author (hereafter, Author 1) compared findings across all groups. One important step was to explore similarities and differences between the group’s answers on the same topic.
- Define and name themes. Step five was a back-and-forth process involving mutual reflections by the researchers involved in coding, and further discussions of findings with Author 1, resulting in the final form reported in this paper.
- Produce a report. Author 1 initiated writing the thematic findings, with all other authors involved in an ongoing commentary on the writing as it evolved (Braun & Clarke, 2006).
Table 1. An example of the analysis (theme 1)
Findings
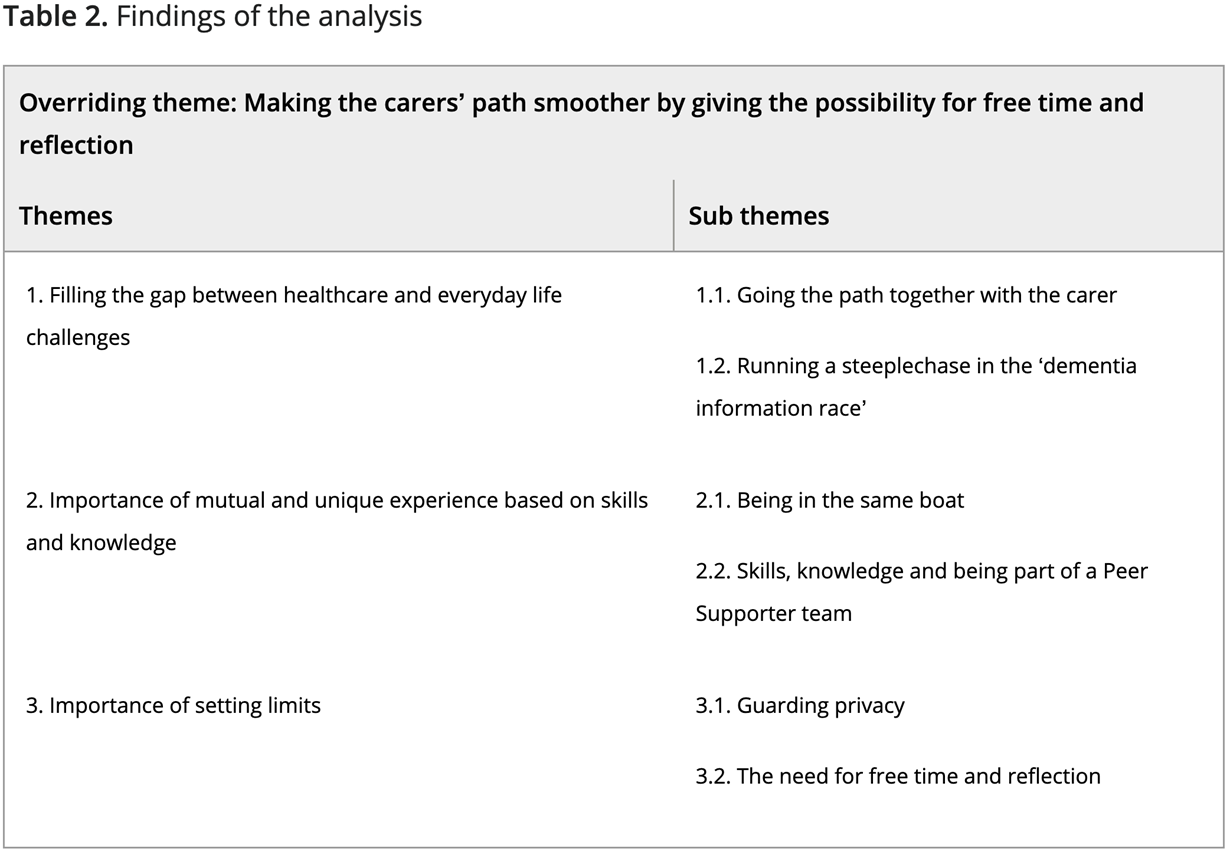
Data analysis identified one overriding theme: Making the path for carers smoother based on their own experience and the possibility for free time and reflection. Three themes were explored as follows (Table 2).
- Filling the gap between healthcare and everyday life challenges
- Importance of mutual and unique experience based on skills and knowledge
- Importance of setting limits and not getting burned out
Table 2. Findings of the analysis
The following section considers each of the themes in more detail.
Theme 1: Filling the gap between healthcare and everyday life challenges
The informants compared what they were able to provide as Peer Supporters compared to what the healthcare service provided. They emphasised their unique contribution, which they perceived as better than services delivered by the traditional healthcare system.
Subtheme: Going the path together with the carers
The informants paraphrased their roles as ‘going the path together with the carers’ by emphasising the importance for the new carers to receive health information:
“…but the information path for the carers can be very long” (Focus group (FG) 1).
They also said:
“We do not answer medical questions” (FG 2).
“…but we need to guide the carers to find their own path” (FG 1).
The informants used their experience as having been carers themselves to guide the carers, as described by one of the informants:
“I think about when my parents lived and were diagnosed. The only information I received was at the hospital. They just said that they had been diagnosed and that I had to inform my other siblings, then. But still you just did not know what it was and how to search for more information, then I said, ‘Do you have something I can read?’ ‘No, you’ll just need to search online’, they said. I were terrified, I did not know what it was, I was wondering ‘Do they die of this?’ And then later on I thought that I will make a difference and help others to make the path easier for the other ones” (FG 1).
Subtheme: ‘Running a steeplechase in the dementia information race’
Being a carer is described by participants ‘like running a steeplechase in the dementia information race’ (FG 1). Carers experienced a lack of understanding among healthcare workers of the changes in the behaviour of a person with dementia. Our informants perceived that some of the behaviour and psychological symptoms of dementia is still associated with shame and is perceived as a private matter. Our informants requested a total package of information about having dementia in the family. They reported that carers only receive fragments of information from the healthcare system. Municipalities within the same health care region offer different services, and obtaining information about a particular dementia service in their own municipality is reported as tricky. Our informants exemplified this by sharing stories about guiding the carers as to who might be the best healthcare provider within their particular municipality. They even talked about how they consulted the healthcare professionals together with the carer, and guided the carers in writing complaints to the healthcare system. One informant also talked about frustrations caused by inadequate healthcare:
“Many also need to rework frustrations of the experience with health care workers’ handling and inadequate information, even it is large pressure about next to kin as being an important resource. It seems that they have not fully realized that carers need information and knowledge about different coping strategies……,and how to get relief to live as good as possible based on their situation” (FG 2).
Furthermore, they also highlighted their responsibility to influence politicians:
“We need to practice reality orientation of politicians” (FG 2).
Another said:
“I perceive that many politicians do not want to see suffering—they do not have so much social conscience if they are not affected by it themselves” (FG 2).
Theme 2: Importance of mutual and unique experience based on skills and knowledge
The informants described the importance of mutual skills of a carer as:
“We are all novices of being carers of people suffering of dementia” (FG 2).
At the same time, the informants underlined the importance of knowledge among Peer Supporters about communication and the training course performed by the Norwegian Health Association.
Subtheme: Being in the same boat
The informants highlighted their unique skills from having been through a period as a carer of a person with dementia. One informant described these mutual skills as:
“A Peer Supporter is one who is in the same boat as the carer, so you have the shoes on, you know what they mean and they almost do not have to say something, because you sense it immediately that here’s someone who really knows what they are going through. It’s like everything else in life, you share special interests” (FG 1).
Another important skill is the ability to see the person with dementia in light of his or her life span and not as a ‘sick’ person. The experience as a carer also depends on the relationship with the person with dementia, whether it be a spouse, son, daughter or any other relationship (FG 3).
In addition to having some family relationship with the person with dementia, they suggested that a Peer Supporter should be of the same gender and age as the carer. They commented that this is difficult to fulfil in rural areas; moreover, how and where they meet the carer differs, depending on the possibility to meet more or less anonymously. Furthermore, in rural areas they are more or less Peer Supporters in different settings and also Peer Supporters for their friends. Therefore, they claimed that the Peer Supporter must be flexible regarding meeting places.
Subtheme: Skills, knowledge and being part of a Peer Supporter team
Our informants were concerned about how to use their own experience in a gentle way without being paternalistic. They did not talk directly about their own experiences and cases but used them to ask questions. These skills are partly autodidactic and partly learned through education as a member of the Peer Support Service in the Norwegian Health Association and in collaboration with other experienced Peer Supporters. They highlighted the importance of taking a certain time before they entered the Peer Support Services, as one said:
“I think there is a big difference between being a Peer Supporter who is still caring for a person with dementia, compared with those who are not. For myself, Mum is gone, and now I’ve got a little more distance. Then it will be a little different than if a spouse, mother or father still lives and you still are an active carer yourself or not” (FG 1).
They needed some time to process their own experience to be able to support others. In addition, knowledge about the disease was pointed out as being important:
“I believe in knowledge, extensive knowledge about more than pills. Understanding that the person has dementia is important, how to interact with someone who has dementia and how to live your own life and take care of oneself all over” (FG 3).
As Peer Supporters, they needed to enjoy meeting and talking with people by phone, face to face and also giving public addresses in dementia clubs, schools and so on. The informants emphasised the importance of overall skills in how to connect with people and using different communication methods such as:
“Recognize them (i.e., carers—authors) while they are talking. Do not interrupt, because most of the time they steer the conversation, as someone mentioned here, they need to talk, simply” (FG 4).
One informant who focused on the importance of being open minded added:
“I think we use common communication theory and guidance questions, just to open up if it’s something they do not say and have difficulty telling, so you often use open questions. They (i.e., carers—authors) say that ‘everything is so difficult, it’s so terribly difficult’ but you cannot get what’s hard. Then I ask, ‘Can you say something about what’s hard?’ It’s important to talk, but it’s just as important to listen” (FG 4).
The informants highly recommended the training course and guidance from a dementia nurse in the National Health Association (2019). These efforts were described as providing a possibility to learn more, to gain valuable support and to form a forum with other Peer Supporters and the dementia nurses to search for guidance and debriefing in difficult cases.
Theme 3: Importance of setting limits
Setting limits is necessary to be able to remain a Peer Supporter over time and for the carer to stay healthy. Trustworthiness seems to be a common feature for both the Peer Supporter and the carer.
Subtheme: Guarding privacy
With their own experience as a carer, our informants explained how confiding to the carers was a moral commitment, while still needing to guard their own privacy. This made the Peer Supporter less risky to confide in than others, including healthcare workers, for example in cases involving violence and sexual acts performed by the person with dementia such as:
“It’s also the case that someone might tell you ‘my man hits me and he has come quite far in his disease’ and so on. What do you do then as a Peer Supporter? Someone I can contact? So, you have to try to convince this person as you talk to them on the phone that they actually need help The carers might say: ‘yes, but shall I begin to reveal to health personnel that my husband has begun to hit me?’” (FG 1).
Therefore, during conversations with the carers, the Peer Supporters emphasised the necessity of seeking treatment for the person with dementia. Furthermore, they needed to take care of themselves and not only care for the person with dementia. Thus, the informants highlighted how hard it was to tell about these episodes of violence while shielding the private life of the person with dementia.
As Peer Supporters, the informants reported that they came to know the carers very well. However, developing a friendship with those who contacted them was rare. One of them described how to keep a distance and maintain privacy by using caution regarding meeting places:
“I try to keep a little distance and set some limits. If they say, ‘Can I come to you?’ I suggest we can meet for example at the volunteer centre. Because we should be a bit careful about talking with them, … you can also be a Peer Supporter for a friend, but I think that some rules need to be set. Otherwise it may get too close” (FG 3).
There was also one example of a carer who considered the Peer Support Service as a public service and expected to have a legal right to phone the Peer Supporter at any time—on Sunday mornings and even on Christmas Eve. Thus, privacy is needed and one participant expressed it like this:
“And if there should be a phone and it is inappropriate, then I’ll tell or ask if they have the opportunity to call again a little later, …... And if I feel that it is being very ‘preachy’ to the other, I try to get along with what I’m doing and prioritize it. So that’s just the few times I have to prioritize my time” (FG 3).
Subtheme: The need for free time and reflection
The informants described the possibility of making a difference and feeling ‘paid back’ (FG 3) and ‘adding something to one's life’ (FG 2) by giving the carers a possibility for free time and reflection, that they possibly lacked themselves, as a part of the motivation to stay in the Peer Supporter Service. They described the experiences like this:
“When I run a conversational groups for spouses, they feel that they have a little break, that is, time for themselves” (FG 3).
At the same time, they clarified their own need for free time and for setting limits and having breaks during their voluntary work. One said that conversation with the carer is sometimes very exhausting and the informant needed free time:
“I feel that they are calling from both the north and the south of the country at the same time as I meet carers on the street at home: they found me online. And I have a conversation group with carers, and after the group meetings they make contact and ask if they can talk with me. Therefore, after the meetings I am very exhausted because it’s very intense and very demanding, the stories they have to tell” (FG 4).
This point was underlined by another:
“I have noticed that if I have had a phone call lasting two hours, you are lost afterward” (FG 1).
Regarding the informants’ own need for free time and reflection, one said:
“I cannot respond to everything, but I can get answers to most; however, in some cases they had to contact others and I referred them to someone else” (FG 4).
In addition, regarding the expression of emotions, the informant highly recommended making distinctions between their own and the carer's feelings:
“Yes, you have to be prepared for everything, and then you have to tighten up so that your own feelings do not take over. It is important….I have to take care of my own feelings and really process them, I move forward and I am able to make sound, independent decisions and communicate with others who are in an emotional situation that I can recognize and respond to. I have to accept the feeling, cope with my own feelings and not transfer them to others. Being emotionally clear is important for becoming a good person. I have to see the other person and think that he or she is an expert in their own life, but might need someone to talk with about thoughts and feelings” (FG 2).
Free time was seen as enabling them to regain power and to reflect upon their own experiences and to cope with their feelings as former carers.



 I helsetjenesten
I helsetjenesten


