Findings
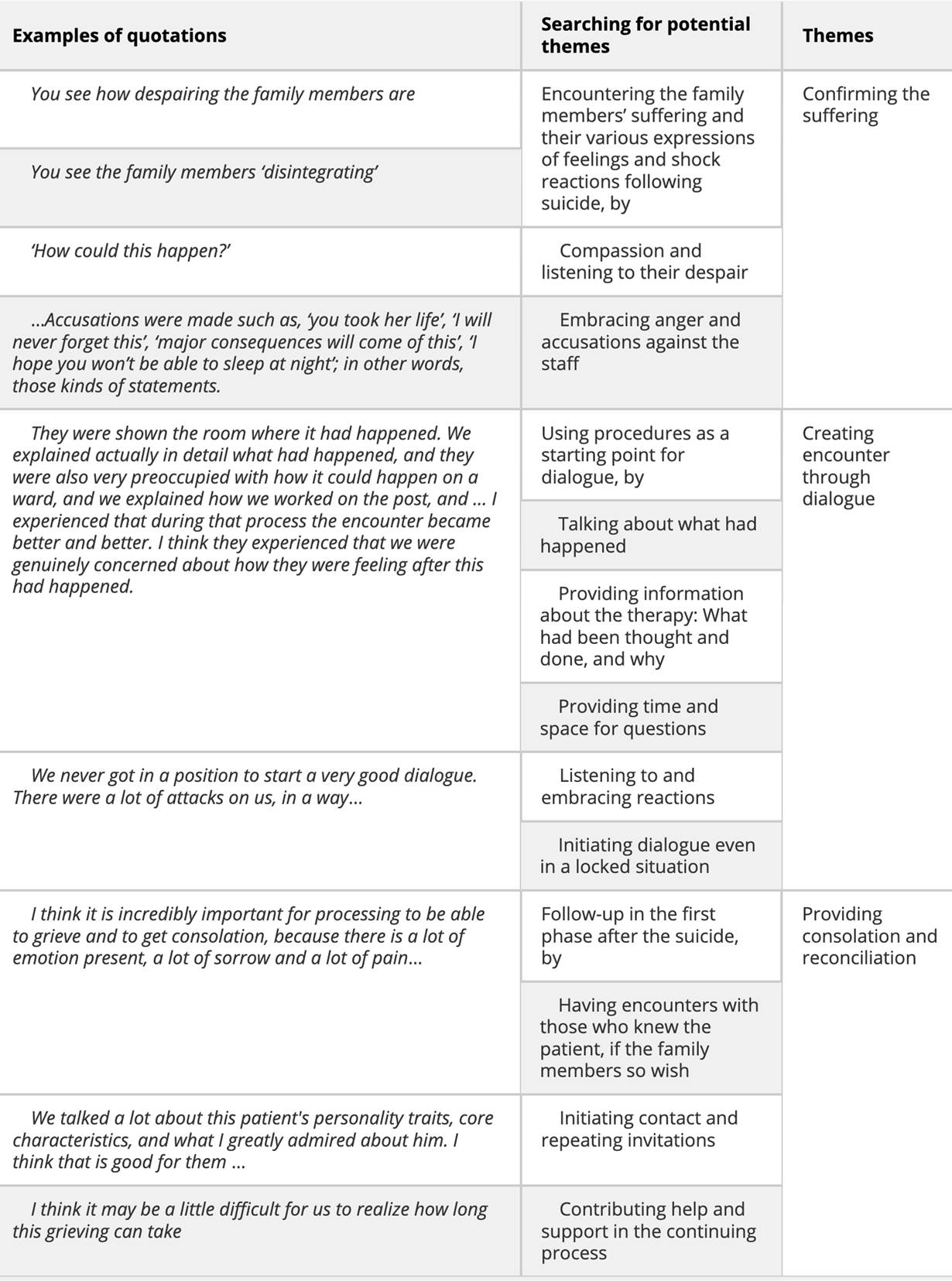
In this study, three themes emerged from the text: (1) Confirming the suffering, (2) Creating encounter through dialogue, (3) Providing consolation and reconciliation. The themes illuminate how MHCPs understand their responsibilities and how they act in the encounter with family members bereaved by suicide. The themes are presented and documented by summarized texts and selected quotations.
Confirming the suffering
This theme is about encountering family members’ shock reactions and feelings in the first phase after a suicide. The participants attempted to confirm suffering by listening to, embracing and tolerating what is expressed. The suicides occurred either during leave from a psychiatric department, just after discharge, or while on the ward itself. In cases where the suicide occurred on the ward, the drama of crisis management, notifications and coordination of measures were also described, as well as care for the welfare of colleagues.
Participants witnessed family members disintegrating emotionally; quiet weeping, outbursts of despair, speechlessness, anger, accusations and threats against staff members. One participant described a first encounter with a family:
First, they were in shock and completely shattered and in despair. And then they were also quite angry. That is, one parent was angry, the other was more emotionally hurt. Or, they had different ways of expressing it. And then the siblings also reacted in different ways. (Participant no.5)
We didn’t see that coming, the participants said about suicide in which they had the responsibility to follow up the family members. It is actually not possible to predict suicide, one of the participants said. Suicide risk is assessed for all patients, … but all in our wards have risk factors. Fortunately, few of them take their own lives. In some suicides the patients might have talked about not wanting to live, but then there were many other things in their accounts that spoke in favour of their wanting to live, the participant said. Then there are others, who don’t take their own lives. These, the participant said, vent much of the pain that they can’t bear to keep to themselves. And we worry about them, from time to time. Suicide and the encounters with family members who were left behind affect the participants: It’s tragic when that is the result you get. This is what we are constantly working to avoid. It’s really tough; we’re just people working here, as one participant put it.
The participants primarily described meetings with a lot of aggressive communication and in which there was a lack of dialogue with family members, or the encounter was complicated. It was a terrible conversation. We were completely ‘exhausted’ afterwards, said one of the participants about such a meeting. Another participant talked about a conversation with a similar starting point: Intense anger and accusations, and occasional attacks. The family had been very concerned and worried about the patient without explicitly mentioning suicide and were critical as to whether the staff followed up the patient closely enough. Therefore, they went into the meeting somewhat forewarned,
but I was in no way prepared for how intense and how… I would almost use the word ugly… that the attack was; that is, personally directed at my colleague. …Accusations were made such as, ‘you took her life’, ‘I will never forget this’, ‘major consequences will come of this’, ‘I hope you won’t be able to sleep at night’; in other words, those kinds of statements. (Participant no.6).
The participant described the emotional statements as ‘attacks’ that continued in the next meeting as well. They were unable to have a good dialogue with this family, and they were soon scheduled to be followed up by others. One of the family members later asked for a conversation, and the participant experienced that they had a good dialogue. Several of the participants relate situations having about the same starting point: intense anger and accusations against the staff for misevaluating the patient and the situation, and threatening statements like ‘you probably know that this is going to have huge consequences’, but where the outcome was different after the process was given some time.
Creating encounter through dialogue
The participants mentioned conversations with parents, spouses, siblings, children, grandparents and other relatives after a suicide, during which they tried to establish a climate for dialogue. They seemed to use points in national guidelines and local procedures as the point of departure for this type of conversation. One participant told how they worked through five or six meetings with a family after the suicide, which started initially with intense anger toward the staff:
They were shown the room where it had happened. We explained actually in detail what had happened, and they were also very preoccupied with how it could happen on a ward, and we explained how we worked on the post, and … I experienced that during that process the conversation became better and better. I think they experienced that we were genuinely concerned about how they were feeling after this had happened. We talked a lot about how it could happen, what our thoughts were about it. We also stated quite clearly that just like when a patient is admitted with cancer or a heart attack, mental health care likewise cannot guarantee a cure for everything. (Participant no.6)
The above quote reflects repeated meetings that contained factual information and gradually encounters where two parties talked together about the suicide from the perspective of both parties. Another participant, however, reported conversations in which dialogue was never established:
We never got in a position to start a very good dialogue. There were a lot of attacks on us, in a way. We are prepared for that; after all, it does happen occasionally, but … We had a conversation with other members of the family afterwards. And they also had a lot of questions, but this time we were allowed to tell our story and how we experienced the incident, what treatment we gave, without constant interruptions and without being contradicted about everything that we said. We established a dialogue; we were able to talk about the patient and about the treatment. We were able to say what we wanted to say, and they could express what was on their mind. (Participant no.3)
When they experienced being unable to achieve the dialogue they strive to establish, it felt to them as if they had lost the opportunity to give family members something they thought could help them later.
No one has learned how to deal with such crises. The statement comes from a participant who claims, based on crisis theory, that it is unlikely, after a suicide, that bereaved will be able to absorb everything they are informed about:
They don’t know exactly what they need to talk about, either. What about ensuring that they know about LEVE (The Norwegian Organization for the Suicide Bereaved)? That’s not exactly one of the things you say in the first conversation. What about children, care support groups? What about family counselling services? And in an initial conversation, you don’t have a chance to convey this. (Participant no.2)
To inform family members in shock about various emergency services in a first meeting was not perceived by the participants as either possible or professionally responsible. They sought first to confirm and embrace their suffering and to build confidence as a basis for dialogue.
Providing consolation and reconciliation
The participants talked about encountering family members following the patient suicide as experiences that had affected them emotionally. They described follow-up of the bereaved by suicide as a task they prioritized. They expressed a wish to provide something, either emotional or practical, that could help the bereaved to progress in their grieving process. The participants mentioned examples of support such as help to contact a close friend in the crisis, to submit their case in a written complaint to the County Governor, or to ensure that bereaved children in a family were followed up. Consolation was one of the care components that was highlighted:
I think it is incredibly important for processing to be able to grieve and to get consolation, because there is a lot of emotion present, a lot of sorrow and a lot of pain. And then I think that consolation may be at any rate the right thing at the right time. (Participant no.5)
Most family members wanted to talk to someone who had known the patient, the participants said. In some cases, the participant had had a longer relationship to the patient who had committed suicide. This allowed them to tell how they perceived the patient and assessed the situation. The participants described examples of messages in which they had shared their personal opinions about the deceased. He was a wonderful person, a really nice guy, one participant said about a patient who had committed suicide. We talked a lot about this patient’s personality traits, core characteristics, and what I greatly admired about him. I think that is good for them, the participant added.
In some cases, follow-up was described as lasting over two years, or extending over three years with less frequent meetings over time. I think it may be a little difficult for us to realize how long this grieving can take, one of the participants said. They gave examples of how grieving moves in waves and that many bereaved by suicide take advantage of the offer to be in contact. So they were keen to convey that the door was open, as in this case:
… I think the pain this parent is left with is quite heavy. That’s why they won’t let go of me but want us to meet from time to time. And so I just say, ‘OK, let’s do that’. (Participant no.2)
Several of the participants had examples of long-term work for those who are bereaved by suicide. They had experiences with family members who struggled with questions for a long time after the suicide. Follow-up at the hospital where it happened provides opportunities for follow-up that they otherwise don’t have, one participant said, as in this case:
So I’ve asked the doctor from here to join our conversation, because a grandmother needed to talk more about what happened and about the treatment. And of course, you can do much better when they have contact with people here where the treatment took place. So if you think of the case as the patient who died, and then having several children, the public health nurses, family counselling, with each and every one, with several other people, with children, with the department head, with the doctor involved in the treatment; all of this is not written down anywhere. (Participant no.2)
This participant reported that they made brief entries in the deceased patient’s chart, but it does not appear in any procedures or codes or interventions, or maybe not at all.
Participants emphasized the importance of professionals initiating contact with family members and repeating the invitation:
If they say, ‘No, we have so many; we have good support’ and so on. Then I think we should say, ‘OK, listen, we’ll call you after a month and find out how things are going with you.’ That’s what we should do. We shouldn’t say, ‘You can just call us’. (Participant no.2)
The participants mentioned the use of SMS and E-mail to remind families that they are still welcome to come in for conversations, even though the use of those kinds of communication media goes beyond the department guidelines. When dialogue in the critical phase following a suicide fails, it is considered particularly important to lower the threshold for contact.
When is enough follow-up? is the question asked by one participant, who mentioned a spouse who reported that he was now receiving good follow-up and that the children were well taken care of: He states clearly that from now on I will no longer need to contact him. But I can imagine that the threshold for getting in contact is high. The participant therefore considered contacting the spouses in a few months’ time. We always end contact with the bereaved after a suicide by saying that we are here, and it is possible to contact us again. They have experienced that even in cases where staff members have made every effort, relatives may still later report that they did not receive sufficient follow-up. You have to stop at some point, but it can be difficult to know where the limit goes for what the relatives may experience as ‘pestering’, in the words of this participant.



 I helsetjenesten
I helsetjenesten

.jpg?x1=0&x2=3500&y1=223&y2=1973&w=1230&h=615&bg=ffffff)