Results
All ten participants were female, ranging from 19 to 30 years of age; only two of them still lived in the family home when the sick parent was diagnosed. Table 2 shows the detailed information on the participants.

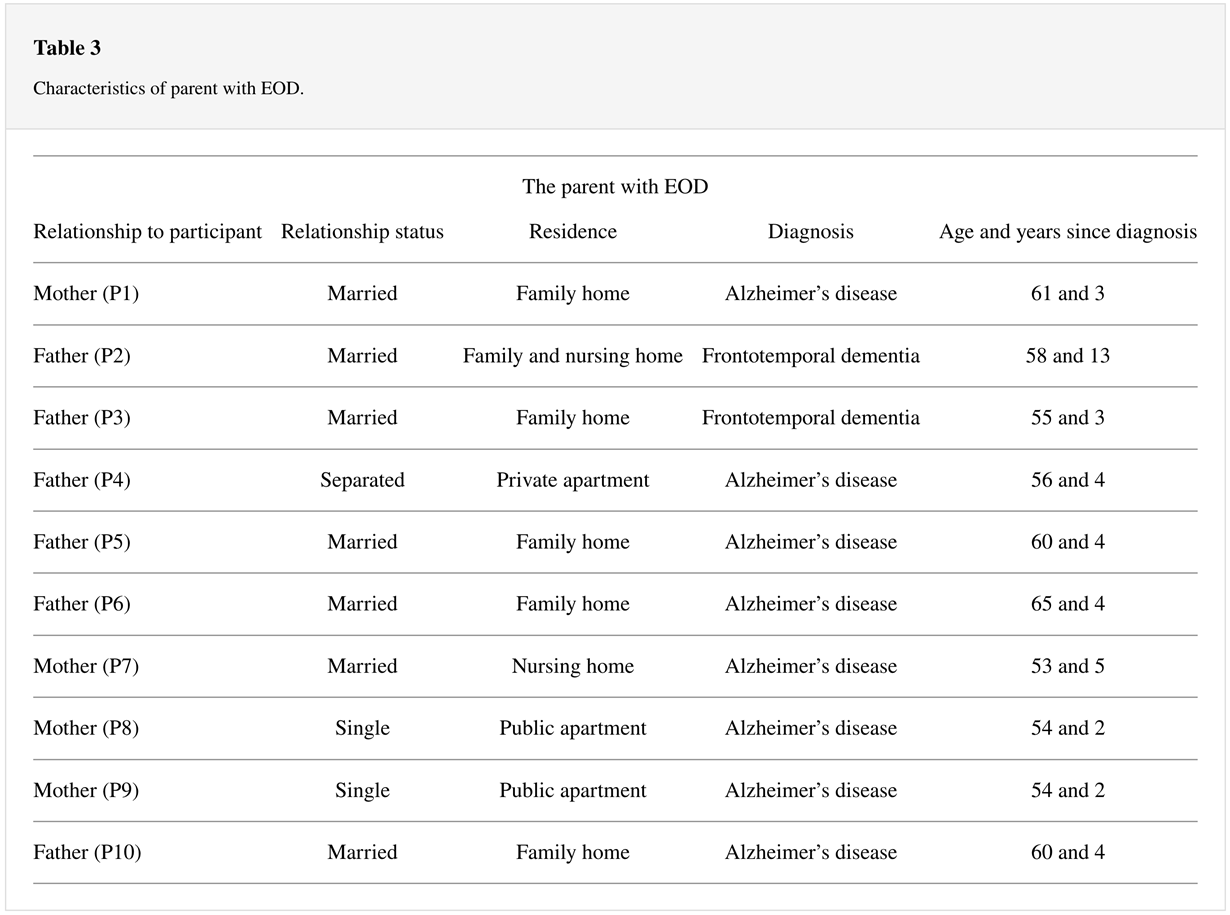
The parent with EOD ranged from 53 to 61 years; four of them were mothers and six were fathers of the participants. Table 3 shows detailed information on the parents.
Themes
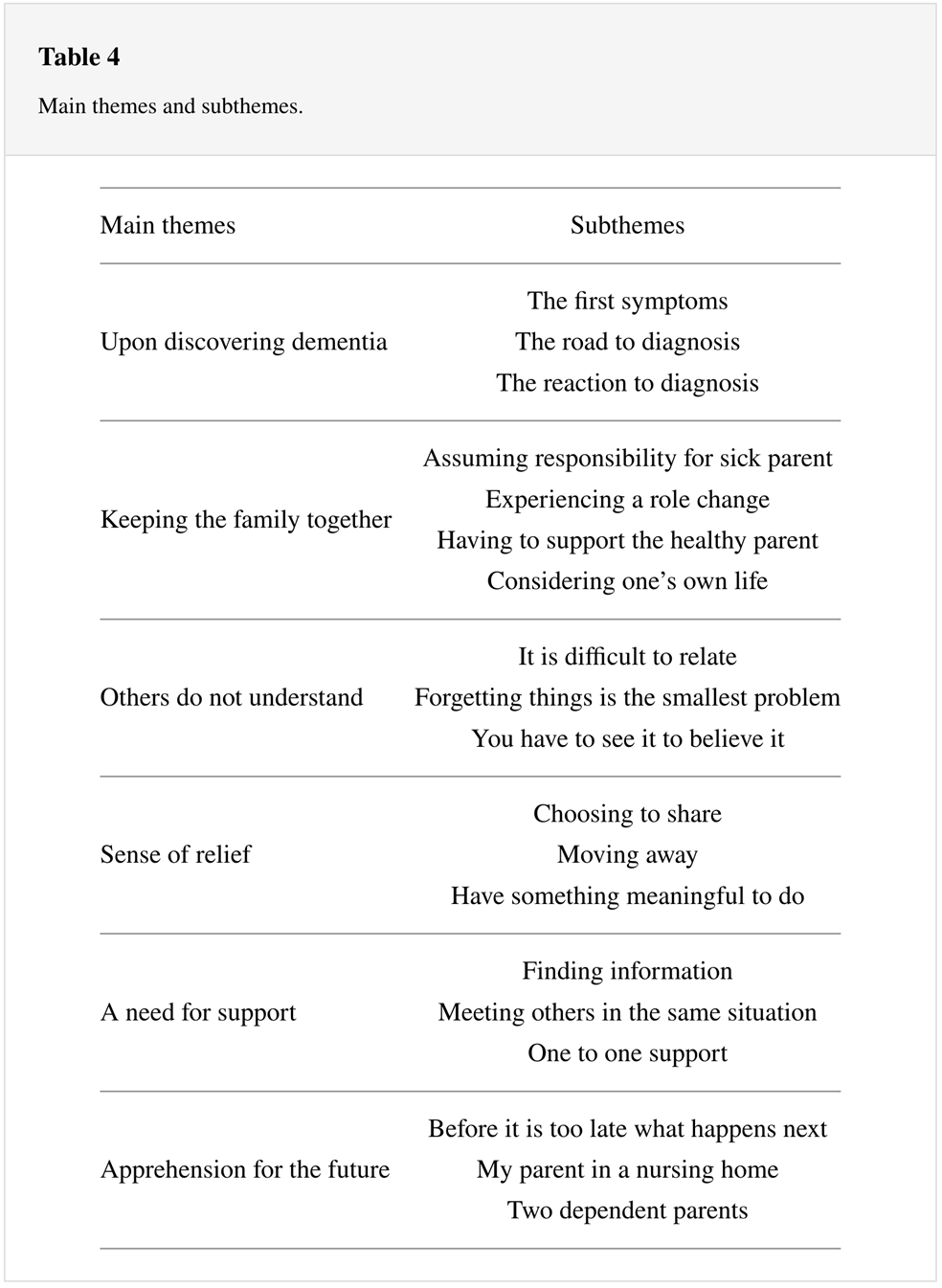
The analysis resulted in 6 main themes and 20 subthemes (Table 4) which described how their parent’s dementia affects the participants’ relationships with family and friends, their personal life, and their support needs.
Upon Discovering Dementia
Some of the first or most frequent signs of dementia noticed by the participants were lapses in memory or mood swings in their parent. The signs were mostly insidious and appeared inconsistently; many participants therefore attributed the signs to other causes like stress or depression. Others experienced more rapid or dramatic changes in their parent, as explained by one participant.
“We were sitting outside eating lunch when all of a sudden, he just took his chair and sat it in between my mother and me and told me “no one comes between us;” he was looking at me like I was some kind of threat (P3).”
First, the road to diagnosis was a period of questioning the changes observed in the parent. Very few participants tried to speak to their sick parent about the symptoms. Some explained that the parent seemed unaware of any change, or that the parent became defensive whenever they were asked about their abnormal behaviour. Some participants said that the family members were divided in their belief that the symptoms were caused by dementia, or as explained by one participant, refused to believe others’ observations and used this as a protective mechanism.
“I was very angry with anyone who implied that my mother had Alzheimer’s and I remember that I could come up with excuses for her behaviour. Even though my sister and father told me that my mother most likely has Alzheimer’s disease one year before the diagnosis, I refused to listen; I did not want my mother to be sick (P7).”
Several participants noted a lack of openness regarding the diagnostic process from both parents and reacted with shock when they were told about the diagnosis. However, accounts of shock and disbelief were also evident among participants who had been more involved in the diagnostic process. Some felt angry, frustrated, or bitter over the fact that someone as young as their parent was suffering from dementia. Others felt a deep sadness; one participant especially spoke of how she right away thought she had to plan for a funeral. For some participants, however, the diagnosis provided a sense of relief.
“It might not be the right thing to say, but it was a relief. Because I now had an explanation for why she behaves the way she does (P9).”
Keeping the Family Together
As the changes in the parent became more evident, the parent became increasingly dependent on assistance. Many of the participants felt that they were needed or obligated to care for their sick parent.
“I feel that this is my responsibility; this is my mother, and I will make sure that she has everything she needs. I feel like I owe it to her in a way, to be there for her, like she has been there for me (P9).”
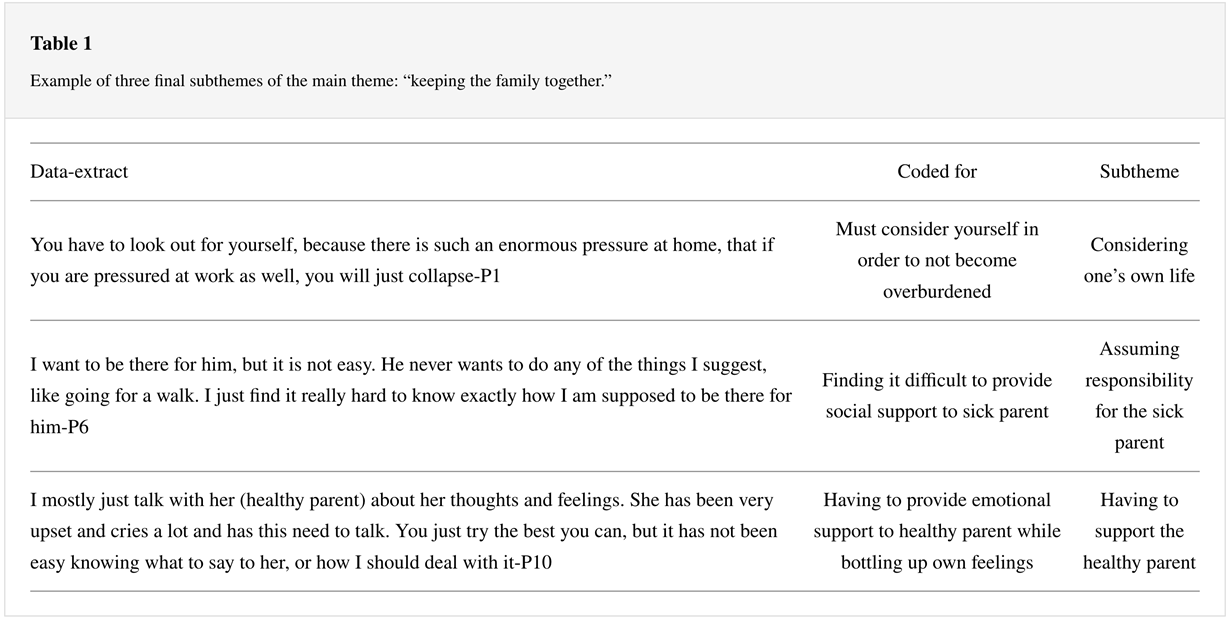
The level and type of care the participants provided for their parents differed, depending on factors such as family structure and functioning, living situations, and level of support from healthcare services. However, it was often not easy to find the best way to identify their sick parent’s needs.
“I want to be there for him, but it is not easy. He never wants to do any of the things I suggest, like going for a walk. I just find it really hard to know exactly how I am supposed to be there for him (P6).”
All participants expressed that their relationship with their parent with dementia had changed. “Everything has changed, she is not my mother anymore; it is an awful thing to say, but I cannot talk to her in the same way I used to (P8).”
The altered relationship not only meant losing a special person, but also a role-change, as the participants felt that they had undergone a transformation from being a recipient of care to becoming a caregiver.
Even though most spoke about the role-change in negative terms, some also stated that the parental illness and subsequent role-change had some positive aspects, such as increased maturity and improved personal qualities. The participants not only provided support for the sick parent, but also most found it equally important to support other family members. Some participants raised concerns regarding the health and wellbeing of the other parent, and there seemed to be a sense of duty to provide support in order for their healthy parent to be able to maintain their dual role.
“When our father told us that he wanted to take some time-off one weekend, we (siblings) right away supported and encouraged him to go and told him “We will take care of her, go and have fun.” When he came back, he felt more energised and could be a much better father to us and husband to my mother (P7).”
As expressed above, the feeling of cooperating and openly communicating with each other to support the healthy parent, or each other, was significant; as a result, some participants stated that they had become closer to their healthy parent and/or siblings. In contrast, some participants spoke of how tension between their parents, small family units, family members who withdrew from the situation, or lack of support from healthcare services, left them with more sole responsibilities.
The participants described, in various ways, how their increasing concerns and/or needs of their sick parent and/or other family members impacted on their personal life and mental state. Some felt that they never had time or energy for their social life, or stated they had to postpone their plans for higher education or even marriage. It seemed like the overall feeling was that their own lives often clashed with the needs of their sick parent and/or other family members.
“It is very tiring because you have a constant bad conscience whenever you do something else. I have in some sense gotten used to it by now, but you do have a bad conscience all the time for not doing enough (P6).”
Others Do Not Understand
When others learned about their parent’s diagnosis, many participants had met with reactions of shock and disbelief. It seemed to be a common experience that others felt uncomfortable speaking with participants about their parent’s illness, which led some to feel unsupported or not understood.
“I think that they do not understand what it means to have a parent with dementia. But they do not talk to me either, it seems that they do not know how; instead, they just completely avoid the subject (P10).”
In contrast, a few participants noted that they felt lucky to have persons in their social network who either were knowledgeable of dementia or had similar experiences of parental illness and who could provide them with a kind of emotional and instrumental support that others could not.
That their parent would only become a bit forgetful was a frequent misconception that the participants faced from others. “Others do not understand how it feels to be a child and see your parent have these episodes of total confusion, or how he can get very angry, childish, and show little sympathy; they do not know that this is happening, they only think you become a bit forgetful (P4).”
Even though this lack of understanding has resulted in loss of contact with friends and/or family members for some participants, they expressed that they in some way understood them.
“I think it has been difficult for people because the illness is a bit invisible before you get really ill, it is not like cancer where you can really see that you are sick (P6).”
Some Sense of Relief
Some of these negative reactions and experiences were reported to cause some participants to feel reluctant talking about their parent’s diagnosis. For some, the reluctance to share was also caused by being asked to keep the diagnosis a secret due to the reported feelings of shame by the sick parent. Nevertheless, those participants who chose to be open, or whose parents chose to share their diagnosis, expressed that this provided them with some relief.
“Since we (mother and participant) agreed that I could tell others about the diagnosis, it has become much easier. If you are having a bad day at work, they will know why; you do not have to explain anything even if you come to work looking like a zombie (P9).”
Most of the participants and some of the parents with dementia had moved out of the family home, resulting in a completely altered living situation. One participant, where the sick parent had recently moved out the family home, described her experience.
“I finally feel free (…) and it feels much easier bringing friends home (P4).”
Many stated that their relationship with the sick parent felt less strained after moving away. “I think in general that it has been easier for me when I do not live at home. I feel that I have more energy now because I am not in it every day in a sense. When I do come home, I feel less irritated by him (P6).”
Their sick parent’s wellbeing was expressed as a constant cause of concern among most participants. It was important for the participants to feel that their parent had something meaningful to do during the day. However, for a daycare offer to be useful, it was important that it was adapted to the sick parent’s needs. When the sick parent had to be in groups of older persons with dementia, they disliked going there, therefore not rendering the same sense of relief.
“It was difficult for me when we were sending him to a place he did not want to go to. I understand that it is difficult to create an offer that fits everyone, but I do not know, it made me feel bad (P6).”
A Need of Support
Following the diagnosis, very few participants were offered an opportunity to talk directly to healthcare professionals or were informed of support offers; many felt forgotten or ignored.
As a result, they had to rely on other family members and most often the healthy parent for information, which was described as problematic in several ways. Firstly, the information the healthy parent received regarding dementia, its prognosis, and available support networks was not always passed on to the participants. “I had to look up things on my own; my father has not been great at asking questions and getting information about what we need to do (P1).”
“Most participants expressed a need to know as much as possible about the progression of the illness, support offers for themselves and their parents. Many said they searched for this on their own and stated that the Internet was a helpful tool. However, being exposed to detailed and unfiltered information about the illness was described by some as a frightening experience. In addition to a need for information, the participants also expressed a need to meet others in the same situation. “To have someone my own age to talk to and learn that their experiences are similar to mine would have been nice, because I have always felt that I am the only one who experience this (P2).”
Those participants that had attended support groups only for young adult children had positive experiences; it is easier to be open with someone in the same situation. However, some expressed a need for one-to-one counselling. “I wish to have someone who will follow up on you, because you are in a very vulnerable situation when you have a sick parent. I know that my father has Alzheimer’s disease and will not be here in the future, but this is a process that takes many years (P10).”
The timing of the counselling also seemed relevant; for some, a meeting with healthcare professionals immediately after the diagnosis was too early, while others found it useful. Nevertheless, all participants expressed that support offers should become more proactive.
“You know how to get a psychologist, but it is a hassle to pick up the phone and do it yourself; if you get this “look here is your appointment, all you need is to meet up,” it is so much easier (P7).”
Apprehension for the Future
The progression of dementia seemed to occupy the participants’ thoughts and a common theme was the uncertainty of how fast the progression of the illness would be. This raised a frequent dilemma of how much time they should spend with their parent while minding their own life.
“I’ve been worried about not spending last Christmas with my father. At the same time, I do not want to worry whether I should spend Christmas with him every year for the rest of his life. That is how you would think about your 93-year-old grandma; we celebrate this Christmas with her because it might be the last (P2).”
Some further expressed how this uncertainty caused stress in their everyday life, as some felt that whenever they had the opportunity, they should go and see their sick parent. Some also said it influenced how they planned and said they would think twice before studying abroad for instance. Another difficult aspect of the progression of the illness was the unpredictability of how it would unfold.
“No one ever told me that he could behave like that (aggressively); I get that, but there is no plan, no “first comes this stage and then the next stage.” I really do not want to think about the future; it just seems like no one can tell me how things will turn out (P4).”
Not knowing how the illness would progress made many participants feel stressed. Another emotional challenge for the participants was that their parent would forget who they are and this appeared to be something that was too difficult to contemplate.
The participants expressed mixed feelings regarding nursing homes. Many felt concerned about whether the nursing home could facilitate their parent’s needs. Therefore, many wanted to have their parent living at home for as long as possible.
“My father will live at home until he does not understand where he is anymore. It is out of the question putting him in an institution now; he will only be left to rot among 80-year-olds. He also walks several miles per day, so if he only has one hallway to walk in, you will have to put him in a psychiatric ward, because then he really needs help (P3).”
The thought of their parent in a nursing home was unimaginable for some and evoked feelings of bitterness and frustration, as it felt unfair to visit their parent in an institution many regarded as a place for older persons.
Another concern was related to the burden of caregiving. Some feared that with the progression of the illness, the demands of caregiving would exceed the healthy parent’s abilities to cope. As a result, some were fearful that not only their sick parent, but also their healthy parent, would become dependent on them, something that would impact their life for the foreseeable future.
“I am really worried about the future. I fear that she will not cope, which means that I have to find a balance of living my own life and being there for her; I cannot take mum with me everywhere though-I am supposed to have a life with my boyfriend too (P10).”



 I helsetjenesten
I helsetjenesten