Methods
We constructed a survey to measure HL and the mentioned outcomes among adult family carers of older person living with dementia across Norway.
Study participants and recruitment strategy
We define a family carer as someone (a family member, neighbor or friend) who, due to the care recipient’s health situation, carries out tasks of a supportive nature that go beyond normal relationships of reciprocity among adults [29]. Persons eligible for the study included any family carer to a person above 65 years of age with suspected, or diagnosed dementia, or symptoms of age-related memory loss. The care recipient could be living independently, in a nursing home facility, or in the same household as the carer.
We obtained a non-probability, opportunistic, convenience sample of family carers by contacting a large number of health personnel, such as those working in local dementia teams, out-patient clinics, nursing homes, and home care service providers, to help with recruitment. They were asked to distribute paper versions of the survey questionnaire, as well as to share a link to the electronic version. They also distributed a one-page information sheet that included a Quick Response code (QR code) that linked to the electronic version of the survey, and were asked to share the electronic link on their web pages or in relevant social media groups. We distributed 410 paper surveys, and 235 one-page information sheets to health personnel for redistribution to family carers. We have no information on the number of family carers who were exposed to information about the survey.
Those who responded online had to provide consent before opening the survey. The information sheet enclosed with the paper version informed potential participants that we considered receipt of the completed form as their consent to participate. All participants were informed that they could withdraw from the study after submission by contacting the research team. No participant availed themselves of this opportunity.
Data were collected between January—May 2019 and the questionnaire was self-administered. Paper-surveys were returned in a closed, prepaid envelope, while electronic forms were submitted online and forwarded to the research team via an encrypted data server.
The Research Ethics Committee judged this study outside their remit as defined by the Norwegian Health Research Act (ref.nr 2018/1725 C). After assessing our data protection and privacy impact assessment (DPIA) and potential risks for participants, the study was approved by the Akershus University Hospital’s Privacy Ombudsman (ref. 2018–126).
Measures
Health Literacy (HL) was measured using the Health Literacy Scale, Norwegian translation (HLS-N-Q12), which is a 12-item, validated scale [30]. Each item is scored on a 6-point Likert scale ranging from 1 = “very difficult” to 6 = “very easy”. Summed scores range from 12–72, with higher scores indicating a higher level of HL [31, 32]. To represent the level of HL as descriptive categories, we converted the 6 levels to 4 as suggested by the scale’s developers, and we followed their procedures for calculating cut-off values [33]. By merging the four middle categories into two middle categories, and applying the cut-off values, the four levels of HL were identified as: inadequate level (score 12–26), marginal level (score 27–32), intermediate level (score 33–38) and advanced level (score 39–48). The 6-level measure was used in the regression analysis, and the 4-level measure in the descriptive analyses.
Carer burden was measured using the Relative Stress Scale (RSS), which has been used to measure such burden in previous dementia research in Norway [34]. RSS measures subjective burden in three areas: 1) emotional distress, 2) social distress, and 3) negative feelings [34]. Each of 15-items is scored on a 4-point Likert scale from 0 = never to 4 = always. Summed scores range from 0–60, and higher scores indicate higher levels of carer burden.
Health Related Quality of Life (HRQoL) was measured using the Norwegian translation of the EQ-5D-5L [35]. This instrument yields two values for HRQoL: a health profile (EQvalue), and a visual analogue scale (EQvas). The EQvalue is calculated by asking participants to rate potential problems in five dimensions of health: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each is rated on a five-point scale with levels of problems ranging from 1 = no, 2 = slight, 3 = moderate, 4 = severe, and 5 = extreme [36]. Each of 3125 possible combinations of responses (health states) is assigned a health state value, the EQvalue, and reported on a scale where 1 is equivalent to full health, and 0 is equivalent to being dead [36]. The EQvas was measured with a vertical, thermometer-like visual analogue scale (VAS), where respondents rated their current health on a scale ranging from 0 = “worst imaginable health” to 100 = “best imaginable health” [36].
Time spent on informal care (Time) was measured using items from the Resource Utilization in Dementia Questionnaire (RUD) [37], adjusted to fit the research questions. This included adding one more traditionally male chore; maintenance of the house, to make the measure more relevant to male carers. We also added time spent talking to the participant on the phone and time spent interacting with health personnel. Tasks were grouped in clusters: 1 = personal care, 2 = gardening, house work, shopping, medication and economy, 3 = talking with the care recipient on the phone, 4 = attending appointments with the care recipient, 5 = interacting with health personnel, or searching for information about services. The time spent on each of the five task clusters were calculated by multiplying the “hours spent on a typical care day” with the “number of days” in which this task was carried out during the last 30 days. The Time variable is calculated by adding up the time spent on all task clusters.
Dementia severity was measured using the Norwegian translation of the Berger Dementia Scale (BDS) to distinguish between those caring for persons living with severe versus mild dementia [38, 39]. The BDS was chosen because it is easy to use, does not demand any medical assessment, and has been used in previous research [40, 41]. The BDS consists of 6 statements that describe different levels of functioning, and asks the family carer which level best describes their care recipient. The statements are ordinal with the first three levels of BDS being classified as “mild dementia” (= 0) and the remaining three as “severe dementia” (= 1), as advised in the literature [39]. We assumed that differences in dementia severity could affect the carers’ outcomes and we wanted to be able to adjust the regression analysis to account for this potential effect.
Socio-demographic variables included age (in years), and gender (female = 0/male = 1). Urban residency was coded on the basis of respondents’ postal code (rural = 0/urban = 1). Highest education achieved was collected as 1 = primary school (9 years), 2 = secondary school (12 years), 3 = Up to three years of university education, and 4 = more than three years of university education. For use in the regression analyses, we distinguished between lower level of education (primary and secondary school, and up to 3 years of university education) and higher level of education (> 3 years of university education), and converted the variable into a dichotomous variable higher education (no = 0/yes = 1). Health personnel was a dichotomous variable, indicating whether the respondent had ever worked as health personnel (no = 0/yes = 1). The variable was included as work experience in the health sector might be linked with higher levels of HL. Carer born abroad (no = 0/yes = 1) indicates whether the carer was born outside of Norway, and was included because earlier studies have shown that immigrants may have lower HL than the other groups [20]. Information about whether the care recipient was living in a nursing home facility or not was collected and the variable was coded as: living in a nursing home facility (no = 0/yes = 1).
Statistical analysis
All analyses were conducted using SPSS version 25 for Windows. All tests were two-sided. Results with p-values below 0.05 were considered statistically significant.
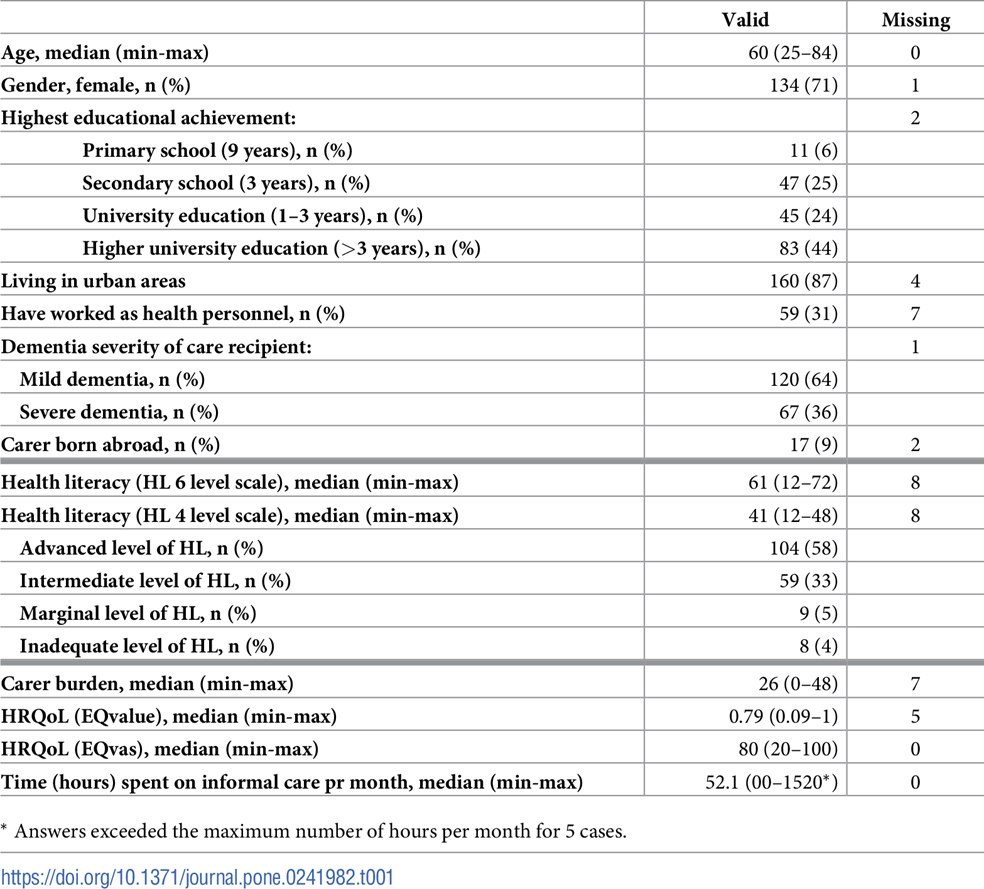
To address our first research aim, we conducted descriptive analyses. We report categorical variables using percentages (%) and the number (n) of valid participants, and the number of missing values. For all continuous variables, we report the median, minimum and maximum values. The median was chosen instead of the mean because the distributions of several variables were skewed, and the median is a better measure of central tendency for skewed data. We chose to present all continuous variables in the same way.
To meet our second research aim, we conducted regression analyses in which the main independent variable was HL and the outcome variables of specific interest were carer burden, health-related quality of life (EQvalue, and EQvas) and Time.
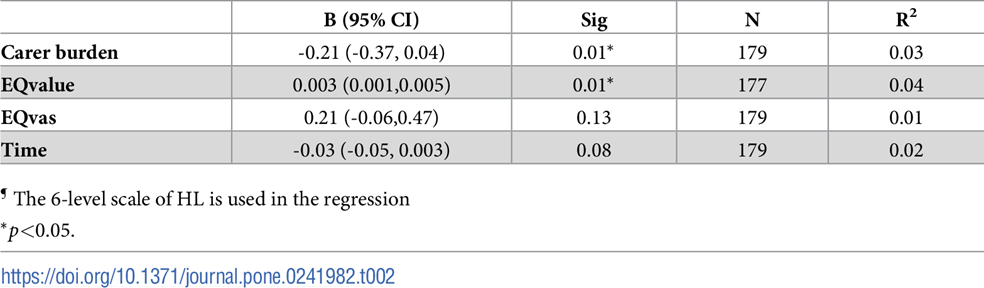
We used bivariate regression analyses to investigate the association between HL and the outcome variables. We then used multiple regression analyses to investigate linear associations between HL and the four outcome variables when adjusting for the effect of the following 8 pre-specified explanatory dependent variables: age, gender, higher education, urban, health personnel, dementia severity, and carer born abroad. The explanatory variables were chosen based on theory, correlation analysis, and the number of cases in the dataset. Imputation was undertaken for missing values for the following three of the variables: HL, carer burden and Time.
For the HL-variable and the carer burden variable; missing values were replaced with a mean value for each case [42, 43]. In those cases were imputation was undertaken, fewer than 3 values were missing.
For the Time variable imputation was undertaken according to the following two procedures: 1) In the few cases where the respondent had answered only one of the two questions used to calculate time spent on informal care, either “hours spent”, or “number of days”, we used imputation of the mean value for the sample. 2) When both values in a cluster of tasks were missing we used the value zero. This occurred in 32 cases. While this included the risk of underestimating the time spent on informal care, it reduced the risk of Type 1 errors in the regression analysis. To test whether this procedure increased the risk of Type II errors, we conducted a sensitivity analysis with imputed mean values.
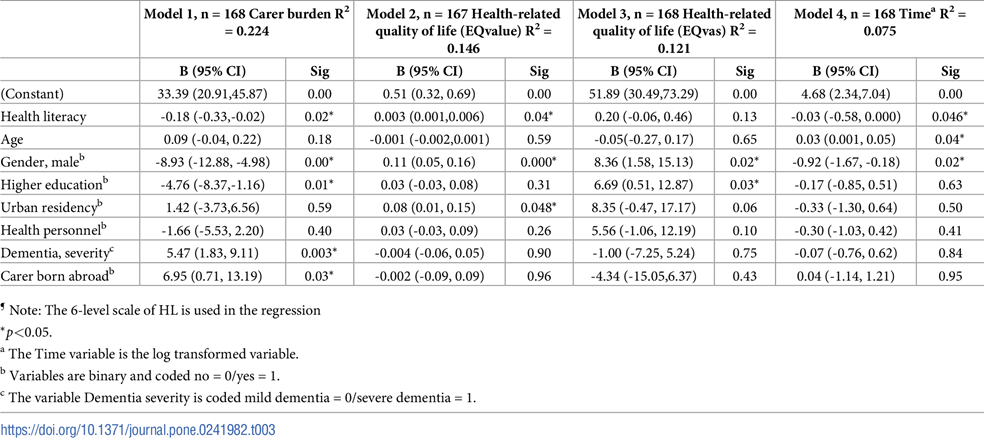
We investigated the associations between HL and each of the outcome variables in the four multiple regressions models: Model 1: The relationship between HL and carer burden; Model 2: The relationship between HL and EQvalue; Model 3: The relationship between HL and EQvas; Model 4: The relationship between HL and Time.
HL, carer burden, EQvalue, and EQvas were treated as continuous variables in the regression models, using 6-levels of HL.
Model assumptions for the multiple regression analyses were tested. All variables except the Time variable had normally distributed residuals. We therefore used log time transformation [42] to meet the assumptions of linearity of the residuals for the Time variable. One minute was added to the total time for each participant in order to avoid logarithms of zero for these calculations. Linearity was checked using scatterplots and correlation analyses. The linearity between HL and the four outcome variables (carer burden, EQvalue, EQvas, and Time) was weak, and for that reason we further investigated the relationship between variables with boxplots of the quartiles of each outcome variable and HL. No other relationship than linear was found between the outcome variables and HL. Homoscedasticity was checked visually on scatterplots, and there was no substantial deviation from normality. There were no multicollinearity issues in the models (VIF < 2).



 I helsetjenesten
I helsetjenesten