Discussion
To our knowledge, this is the first review of the research literature that explores and discusses caregiving motivation from the SDT perspective. In sum, the analysis of the included articles has found that all studies considered satisfaction of the three basic psychological needs for autonomy, competence and relatedness as essential for predicting caregivers' quality of motivation and thus their well-being. The review holds the potential to form an important foundation for future research, and for the development of interventions that will increase caregivers' sense of self-determination.
Caregivers' motivation and well-being in a long-term illness context
The most significant finding was that fulfilment of caregivers' psychological needs and autonomous motivation was strongly associated with their greater well-being. Our findings are consistent with Milyavskaya and Koestner
23 who found that need satisfaction is universally linked to motivation and well-being across important life domains. Other researchers have come to the same conclusion in workplace studies
19, 22, among patient populations in health care, and in health promotion contexts
20. Moreover, Weinstein and Ryan
21 found that intrinsic motivation for helping yielded benefits for the helper through greater need satisfaction. Perception of choice in entering the caregiver role is positively associated with well-being among caregivers, and internalised values about the importance of caregiving are essential
12. This is consistent with our findings, where the maintenance of motivation over time requires that caregiver's internalise certain values, duties, responsibilities and skills. Moreover, this review suggests that the feelings of caregiving as voluntary and fulfilment of the need for autonomy is especially important for high-quality motivation. Also, caregivers' perception of support for their autonomy from family and friends, from their workplace and from health professionals may be associated with less depression and increased well-being and life satisfaction. In line with this, high-quality motivation is a central marker of well-being and associated with high performance
22 and personal growth
20, 21. In extension of this, we see the need for health professionals supporting the caregivers' volunteering behaviour and offering guidance towards caregiving solutions to support sense of autonomy.
Our findings support the theoretical proposition that fulfilment of the basic needs for autonomy, competence and relatedness is a primary form of psychological nurturance that facilitates well-being
17, 18 in caregivers. Intrinsic motivation is distinguished by autonomous motivation and self-determined behaviour where the person acts out of interest, engagement and enjoy the activity
18, 20. The review show that fulfilment of the three basic psychological needs for autonomy, competence and relatedness are important determinants of caregivers' well-being, protecting them from high levels of psychological distress associated with ill-being and caregiver burden. In a job satisfaction context, amotivation, where the motivational quality is lowest and the employee finds no value or interest in acting, is associated with poor well-being and performance
19, 22. The employee appears to have no self-determination and the motivation for acting is controlled, resulting in poorer well-being
17. Our narrative analyses confirmed this by showing that caregivers who reported feeling forced or obligated to offer care were extrinsically motivated or amotivated, which predicted more depressive symptoms, less life satisfaction, and greater stress and caregiver burden.
Targeting caregivers' autonomous motivation
We found that a motivational perspective on helping, as provided by SDT, is useful in explaining variations in personal and relational well-being and distress among caregivers. Early identification of caregivers who are struggling or at risk of struggling is crucial
4. It is important to identify this subgroup of caregivers so that they can receive evidence-based services
6. SDT constructs can identity, clarify and explain why caregivers in apparently similar situations differ in terms of well-being and in their desire to continue offering care. According to Roth et al.
6 it is important to target evidence-based services to the subgroup of caregivers who are under stress or at risk in other ways
6. In line with this, we found that by identifying caregivers who were intrinsically motivated or amotivated and suffering from the caregiver experience, health professionals might better understand why certain caregivers experience worse well-being than others, and how these caregivers will benefit from receiving support services or counselling.
Our results highlight the need for improved ways of supporting caregivers' motivation. Moreover, it is crucial for health professionals to understand when the provision of caregiver support is considered helpful and beneficial for the caregivers' well-being. According to previous caregiver research, health services ought to see informal carers as no less important than the patient
2, 4, 11. Different kinds of caregivers need different kinds of support and interventions based on, that is, types or severity of the relatives' long-term illness
1, 9. Support and services to caregivers are indispensable to caregivers' psychological well-being by preventing burnout
4, 8. This is consistent with our findings that well-being is facilitated by perceived support, especially support for autonomy from health professionals, the patient and from others. Given the critical role of autonomous helping motivation, health professionals can meet caregivers' needs by being autonomous supportive. Promising result from the two pilot interventions in the fields of cancer and heart failure encourage further development and testing of interventions that support caregivers. The interventions recommend that health professionals reinforce caregivers' autonomous motivation by offering choices rather than restrictions, showing the range of options available to them, avoiding criticism and giving encouragement
31, 39. Accordingly, health providers should view caregivers as partners
5, and take into account caregivers' resources
13. Here, a more balanced image of the caregiver as a resilient and capable ally is useful
6. Health professionals could work more effectively and systematically with patients to identify, inform and collaborate with their informal caregivers
6. According to Quinn et al.
10 efficacious interventions should be developed and implemented to support caregivers' motivation and thus their well-being.
Future directions for SDT in the caregiver context
Our findings suggest that models of understanding caregiver well-being ought to focus not just on the absence of stress and caregiver burden, but also consider motivation as the foundation for caregivers' long-term health and well-being. These findings meet previous research calls for promotion of benefits of caregiving, such as sense of satisfaction, autonomy and expertise among caregivers that may act as specific and legitimate goals for motivational support
5, 6, 14, 15. The existing dominance of a stress-coping approach pathologies caregiving
6, 14. In contrast, SDT represents greater attention to health promotion
20 and offers a promising theoretical framework for future research, by shifting the focus from health threat to health resources in the caregiving context.
All of the included articles described how SDT was applied in their respective studies, depicting SDT as an effective framework for understanding caregivers' motivation. In this context, it would be valuable to know more about the application of SDT in research on caregiving, and in particular, qualitative research is warranted to identify the SDT constructs' application in real life. Moreover, all of the reviewed articles included both male and female caregivers, while only two studied SDT constructs with respect to gender
32, 33. The gender issue in current SDT research has provided inconsistent findings
41 representing a knowledge gap in the SDT research on caregiver motivation.
Most of the studies included in this review used SDT measurements and questionnaires validated in or adapted from other contexts. Accordingly, the development, testing and validation of SDT-based instruments and questionnaires in different languages adapted to a caregiver context are warranted. Further development of qualitative research approaches to identify methods of promoting caregivers' autonomous motivation is recommended. This could add value to a field of SDT research that is already dominated by quantitative methods. Future SDT research on caregivers should endorse reporting and reflecting on the application of SDT.
Methodological considerations
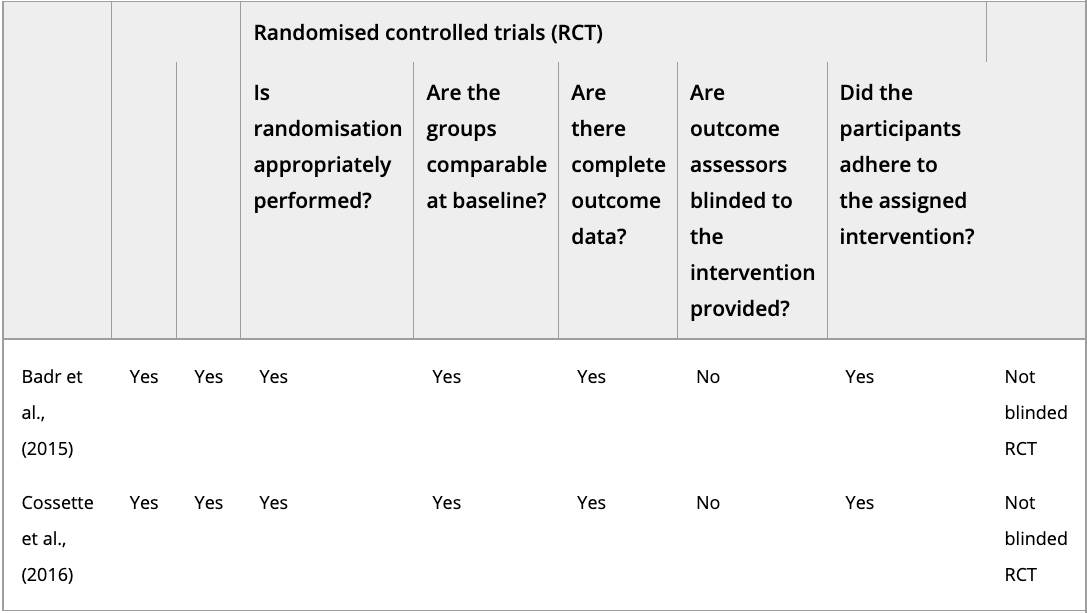
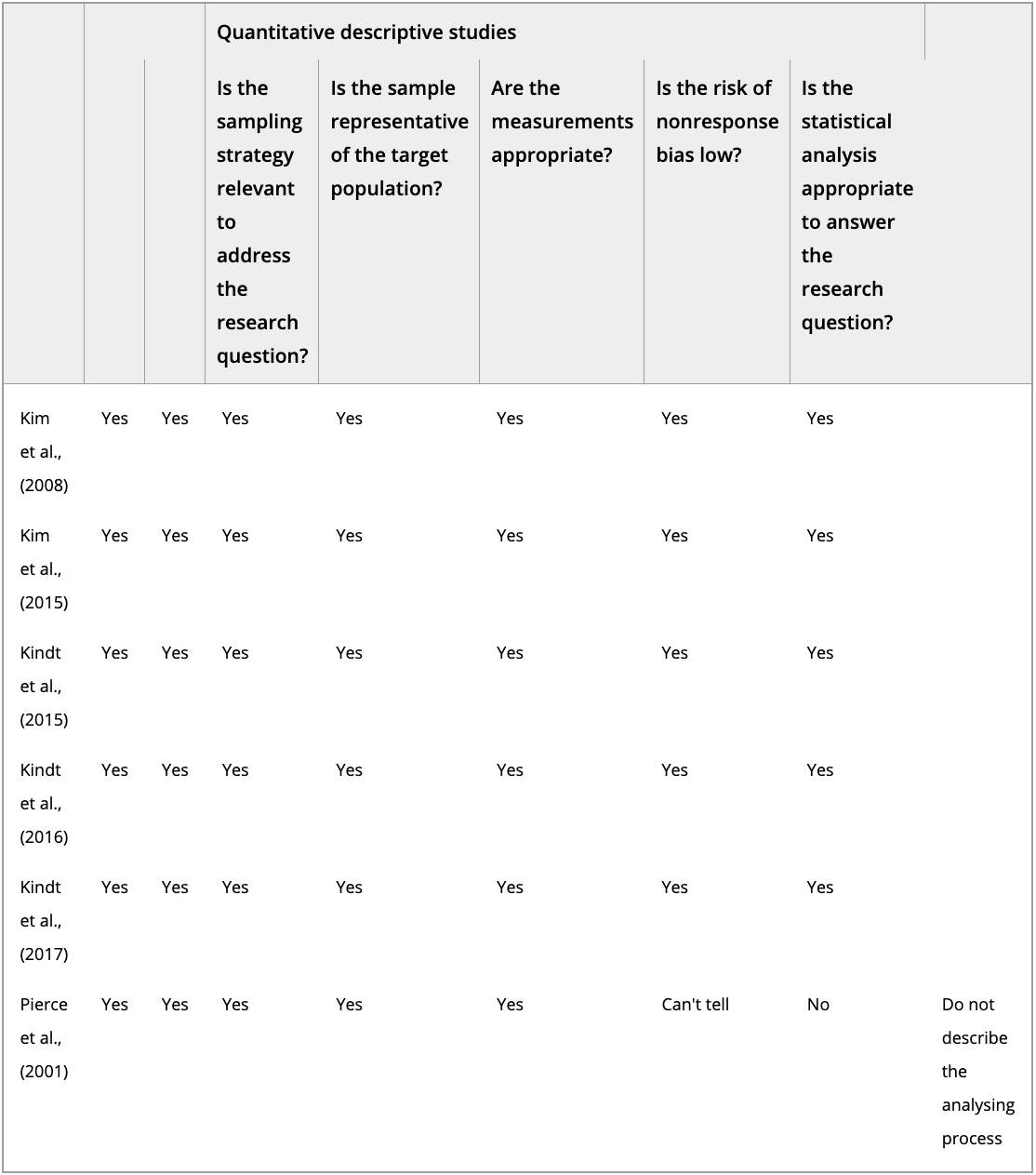
It can be methodologically challenging to include mixed evidence within one literature review. The integrative review method has been successfully adapted to allow diverse primary sources and multiple perspectives to be combined, to gain in-depth understanding of complex phenomena
26. Whittemore and Knafl's integrative review method
24 provided a stringent approach to the current review study, represented by its rigorous and systematic review procedure.
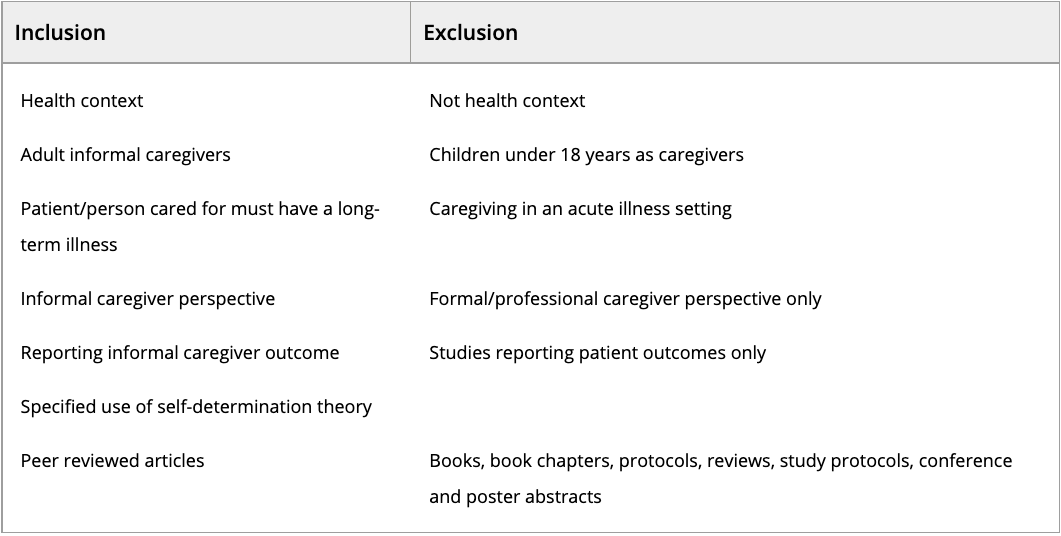
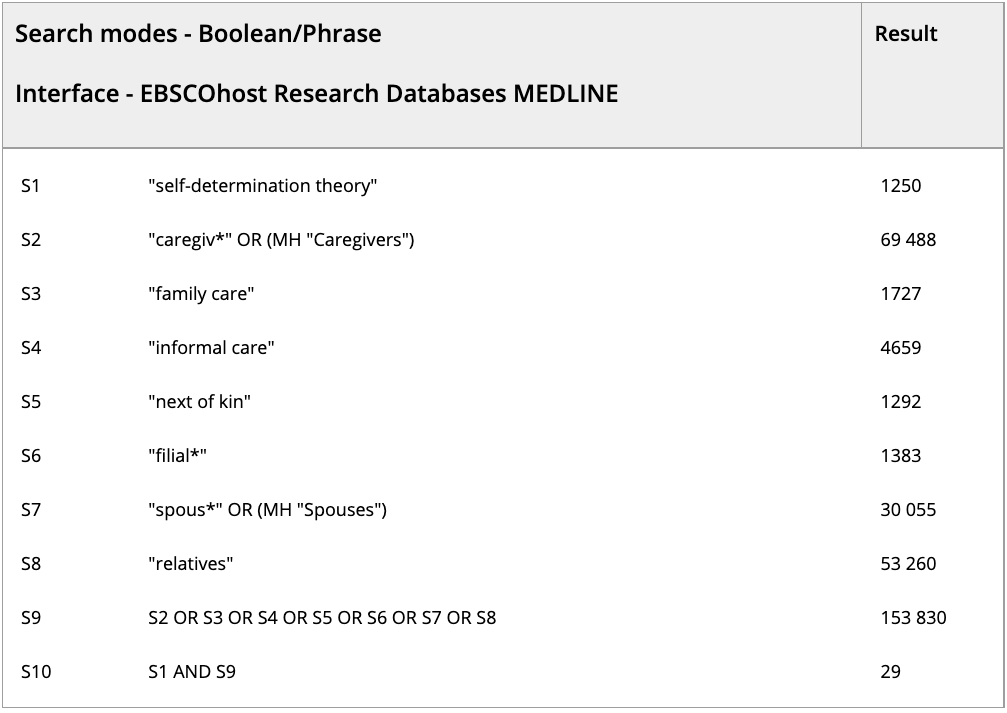
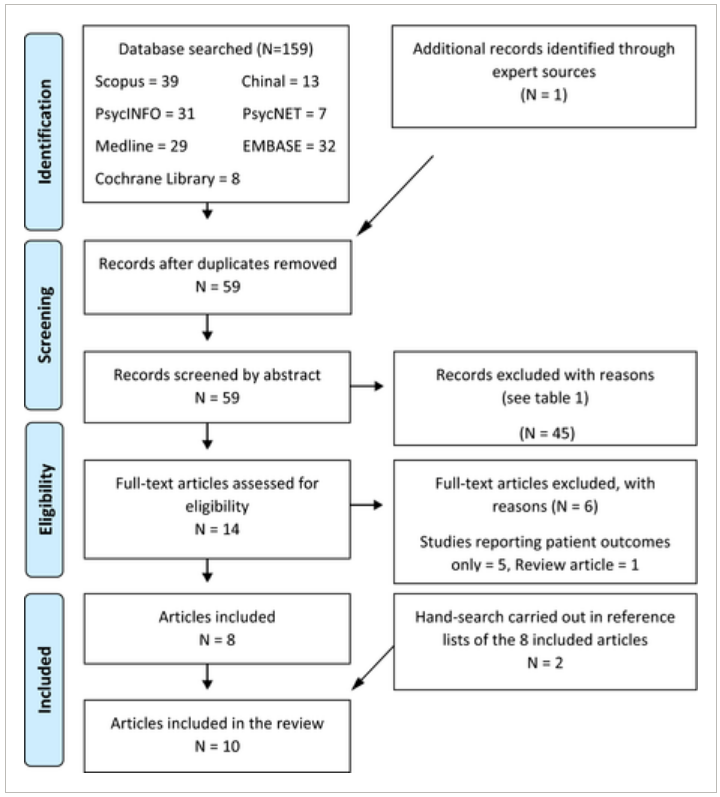
Our search strategy was comprehensive, comprising two searches (initial and follow-up) in seven multidisciplinary bibliographical databases. This allowed for an updated and interprofessional approach to the literature search. Even though no limitations on year or language were added to the literature search, only 159 articles were found, most of them published since 2015 and published in English. This indicates a circumscribed research area, but at the same time the combination of caregiving and SDT seems new and upcoming in both research and practice. Despite a comprehensive literature search, the inclusion of grey literature might have given expanded access to the research area. To enhance the rigor of our review, a priori and well-defined selection criteria were used. All authors participated in study selection, ensuring that the identified documents were eligible for inclusion. Choosing a single motivational theory (SDT) as a theoretical perspective might be considered a strength of this review, but may have narrowed the knowledge base. The inclusion of other motivational theories might have contributed to a broader view on caregiving motivation.



 I helsetjenesten
I helsetjenesten